

Introduction: Despite advances in tyrosine kinase inhibitor (TKI) therapy for chronic myeloid leukemia (CML), there remains a sizeable proportion of patients (pts) with CML in chronic phase who are refractory or intolerant to these agents. A good understanding of the most recent real-world patterns of care in these pts is necessary in order to provide context for assessing the potential benefits of new treatments undergoing clinical development. The aim of this study was to evaluate treatment patterns in CML pts cycling through TKI therapies achieving later lines of therapy, and to estimate their healthcare resource utilization (HRU) and costs.
Methods: Adult pts with CML in the United States who received at least 3 lines of TKI therapy were identified in the IBM MarketScan Commercial and Medicare Supplement databases (Q1/2001-Q2/2019). Treatment patterns were observed from CML diagnosis. Pt characteristics were measured during the 6 months prior to third line (3L) initiation (baseline period). All-cause HRU (inpatient [IP] admissions and days, days with outpatient [OP] services, and emergency department [ED] visits) and costs (medical and pharmacy) were measured 1) during the course of 3L therapy (from 3L initiation to termination) and 2) between 3L initiation and end of follow-up (stem cell transplant [SCT], or end of data availability/health plan coverage). HRU was reported using monthly incidence rates per 100 pts (IR/100pts); costs (2019 USD) were evaluated per-pt-per-month (PPPM) from a payer's perspective.
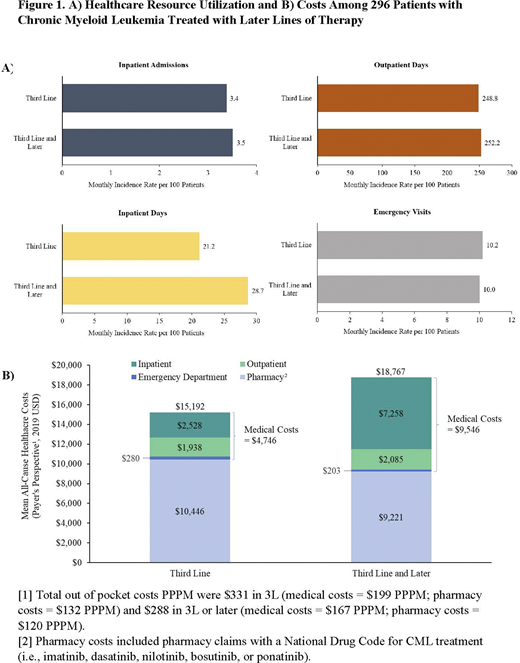
Results: Of the 48,168 pts identified with CML, a total of 296 CML pts initiated 3L therapy; median age was 58.5 years (30% were aged ≥65 years) and 50% were female. The mean follow-up period from CML diagnosis was 57.8 months and from 3L initiation was 24.5 months. Most pts had their first CML diagnosis in or after 2010 (71%) and achieved 3L in or after 2014 (50%). At baseline, the mean modified Charlson Comorbidity Index score (excluding CML) was 1.6 with 24% of pts with a score ≥3, 64% of pts had a moderate or severe Darkow Disease Complexity Index, and the most prevalent comorbidities were hypertension (45%) and diabetes (25%); 21% of pts (i.e., ≥1 indicator of congestive heart failure, cirrhosis, or end-stage renal disease, or ≥75 years old). The most common sequences of TKIs from first line (1L) to 3L were imatinib → dasatinib → nilotinib (28%), imatinib → nilotinib → dasatinib (16%), imatinib → dasatinib → imatinib (9%), and dasatinib → imatinib → nilotinib (5%). The mean duration of 1L, second line (2L), and 3L therapy was 14.9, 10.4, and 15.6 months, respectively; 62% of pts were still in 3L at the end of follow-up. Only one patient received SCT after 3L. The most common TKIs received at each line were imatinib in 1L (65%), dasatinib in 2L (49%), and nilotinib in 3L (36%). The mean treatment-free period (time between line of therapy termination and next line initiation) between 1L and 2L was 1.3 months, 2.6 months between 2L and 3L, and 1.5 months between 3L and 4L. During 3L therapy, pts had a monthly IR/100pts of 3.4 IP admissions, 21.2 IP days, 248.8 OP days, and 10.2 ED visits (Figure 1A). Pharmacy costs accounted for 69% of the mean total costs of $15,192 PPPM, with medical costs accounting for the remainder (Figure 1B). In 3L therapy and later, pts had a monthly IR/100pts of 3.5 IP admissions, 28.7 IP days, 252.2 OP days, and 10.0 ED visits (Figure 1A). Pharmacy costs accounted for 49% of the mean total costs of $18,767 PPPM, with medical costs mainly driven by IP costs (Figure 1B).
Conclusions: This study characterized CML pts receiving later lines of therapy, a clinical population which has not been previously well studied with important unmet treatment needs as they repetitively fail TKI therapy. Although the majority of pts were likely fit for SCT, SCT was rare. In addition, pts quickly switched to the subsequent line of therapy, both facts suggesting that an important proportion of pts were intolerant to previous TKIs. While pharmacy costs accounted for nearly half of the total cost burden during 3L, the proportion of medical costs PPPM took more importance following 3L therapy, with IP costs being the primary cost drivers for this increase. These findings support the need for better treatment options in pts with CML undergoing later lines of therapy.
Atallah:Novartis Pharmaceutical Corporation: Consultancy; Jazz: Consultancy; Pfizer: Consultancy; Takeda: Consultancy, Research Funding; Abbvie: Consultancy; Genentech: Consultancy. Maegawa:Novartis Pharmaceutical Corporation: Current Employment, Current equity holder in publicly-traded company. Latremouille-Viau:Novartis Pharmaceutical Corporation: Consultancy, Other: Dominique Latremouille-Viau is an employee of Analysis Group, Inc. which received consultancy fees from Novartis.; Sanofi Genzyme: Consultancy, Other: Dominique Latremouille-Viau is an employee of Analysis Group, Inc. which received consultancy fees from Sanofi Genzyme.. Rossi:Novartis Pharmaceutical Corporation: Consultancy, Other: Carmine Rossi is an employee of Analysis Group, Inc. which received consultancy fees from Novartis.. Guerin:Abbvie: Consultancy, Other; Sanofi Genzyme: Consultancy, Other: Annie Guerin is an employee of Analysis Group, Inc. which received consultancy fees from Sanofi Genzyme.; Novartis Pharmaceuticals Corporation: Consultancy, Other: Annie Guerin is an employee of Analysis Group, Inc. which received consultancy fees from Novartis.. Patwardhan:Novartis Pharmaceutical Corporation: Current Employment, Current equity holder in publicly-traded company.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal